Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Keyboard shortcuts (Alt+K)
Demographics:
60 years old, Female
Indication:
Acute respiratory failure
Findings
Chest radiograph
- Central interstitial thickening with patchy bibasilar opacities and likely trace bilateral pleural effusions
- Endotracheal tube tip projects 4 cm above the carina
- Gastric suction tube tip projects over the gastric antrum
- Bilateral diaphragmatic pacing wires
CT
Chest
- Widespread tracheobronchial intraluminal debris, particularly in the lower lobes
- Bilateral lower lobe dependent consolidation
- Small right and trace left pleural effusions
- Endotracheal tube terminates above the carina in the midthoracic trachea
- Tiny hypodense nodules in the left thyroid lobe, which are not large enough to require further imaging evaluation
Upper abdomen
- Bilateral diaphragmatic pacing wires
- Gastric suction catheter courses into the stomach
MSK
- T9 compression fracture with approximately 20% central height loss and no bony retropulsion
Diagnosis
Aspiration
Sample Report
Findings consistent with massive aspiration.
Age-indeterminate T9 compression fracture without bony retropulsion. Recommend correlation with point tenderness at this location.
Discussion
- Aspiration can result in a variety of imaging appearances depending on the amount and quality of the material aspirated
- Debris within the airways is a tip-off, but is not entirely specific since airways inflammation (e.g. bronchitis) results in increased intraluminal secretions, which can look identical to aspirated fluid
- Here are some potential imaging appearances:
- Tree-in-bud nodularity: microaspiration fills scattered distal bronchioles and alveoli but not enough to result in confluent opacification
- Groundglass opacities: larger amount of aspiration results in more confluent opacification of adjacent alveoli, although the concentration of aspirate is not enough to completely obscure the pulmonary interstitium
- Crazy paving pattern (patchy groundglass opacities and interlobular septal thickening): patients with chronic repeated aspiration can have shifting areas of groundglass opacification with associated interlobular septal thickening resulting from chronic interstitial inflammation and engorged lymphatics working to clear the aspirated material
- Consolidation: even larger amounts of aspiration can fill alveoli with high enough concentration to obscure the surrounding interstitial anatomy
Annotated Images & Illustrations
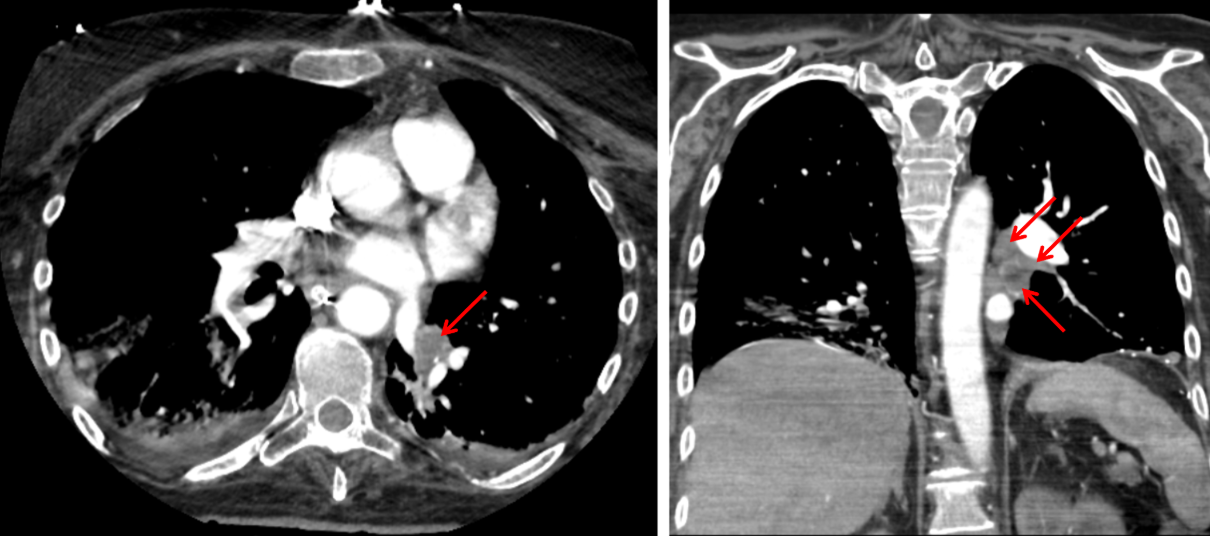
Soft tissue attenuation material filling left lower lobe bronchi (red arrows), most concerning for large volume aspiration.