Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Findings
Lower chest
- Mild cardiomegaly
- Mild dependent atelectasis
Abdomen/Pelvis
- Large fluid attenuation structure in hepatic segments 7 and 8 measuring 10 x 7 x 7 cm with internal septation and circumferential ill-defined low attenuation compatible with edema
- Peripherally enhancing subcapsular collections along the anterior margin of the left hepatic lobe (collection 1, collection 2) measuring 3 x 1 cm and 2 x 1 cm
- Clearly marginated fluid attenuation structure in segment 7 and several other scattered tiny hypoattenuating lesions, which likely represent cysts
- Mild mural thickening of a segment of the sigmoid colon with adjacent fat stranding and a 1.5 cm fluid and gas collection along the tip of an inflamed diverticulum
- Loss of the normal fat plane between this collection and adjacent loops of small bowel, which demonstrate mural thickening
- No bowel obstruction
- High grade stenosis of the left common iliac artery, with the left internal and external iliac arteries remaining patent
- Incidental splenule
MSK
- No acute findings
- Ankylosis of both sacroiliac joints
- Circumscribed sclerotic lesion in the left anterolateral seventh rib without aggressive features, likely a bone island
Diagnosis
Hepatic abscess
Sample Report
Acute sigmoid diverticulitis complicated by a small contained perforation and a large abscess in the right hepatic lobe. Additional small subcapsular abscesses along the anterior margin of the left hepatic lobe.
Additionally, there is loss of the normal fat plane between the peridiverticular collection and adjacent thickened loops of small bowel raises the potential for an enterocolonic fistula.
High grade stenosis of the left common iliac artery. The left external and internal iliac arteries are patent.
Discussion
- Pyogenic hepatic abscesses have many potential etiologies, including:
- Direct spread from adjacent infection (e.g. gangrenous cholecystitis) or external introduction of infection (e.g. penetrating trauma)
- Biliary spread from ascending cholangitis
- Hematogenous spread (particularly from GI infections, as in this case)
- The classic CT imaging appearance is a double target sign with internal low density surrounded by an internal enhancing rim (capsule) and a low density external rim (edema)
- Abscesses may be unilocular or multilocular
- Gas is present in a minority of cases
- Unfortunately, necrotic tumors can have an overlapping imaging appearance, so it is important to follow these to resolution
Annotated Images & Illustrations
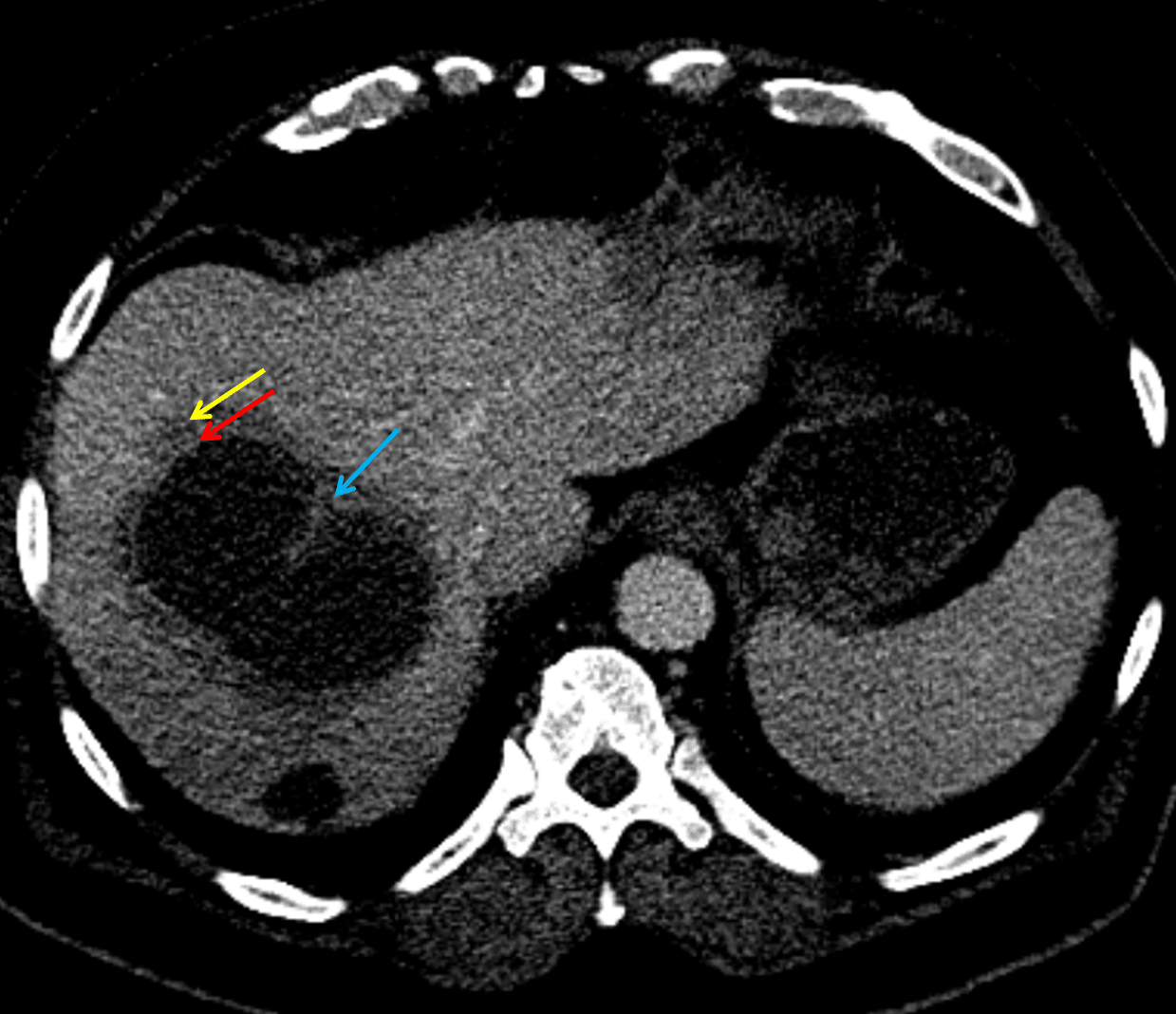
Hepatic abscess showing the double target sign with low density internally surrounded by a thin inner enhancing rim (red arrow) and ill-defined outer low density rim (yellow arrow). Blue arrow indicates an internal septation.
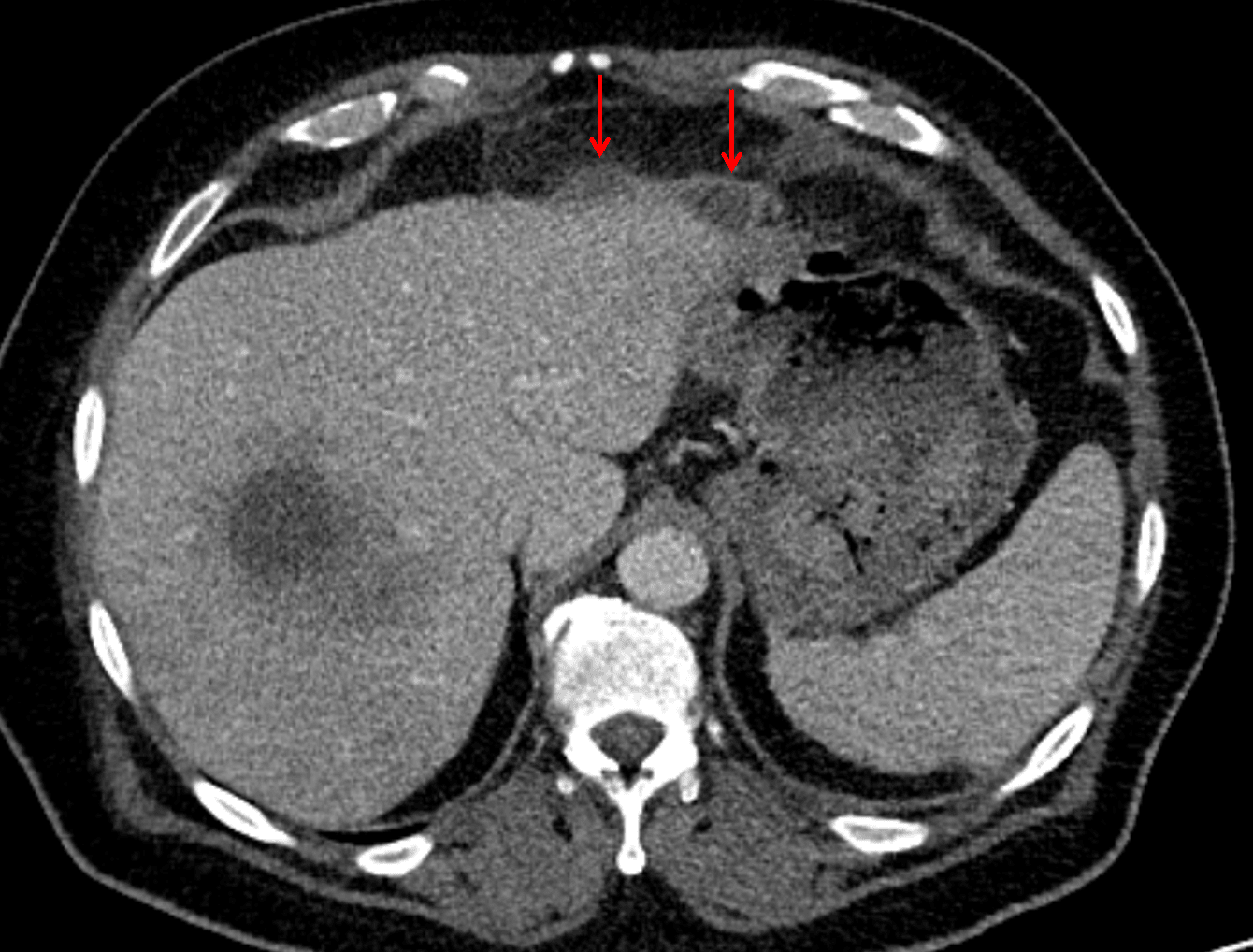
Red arrows: additional smaller subcapsular abscesses.
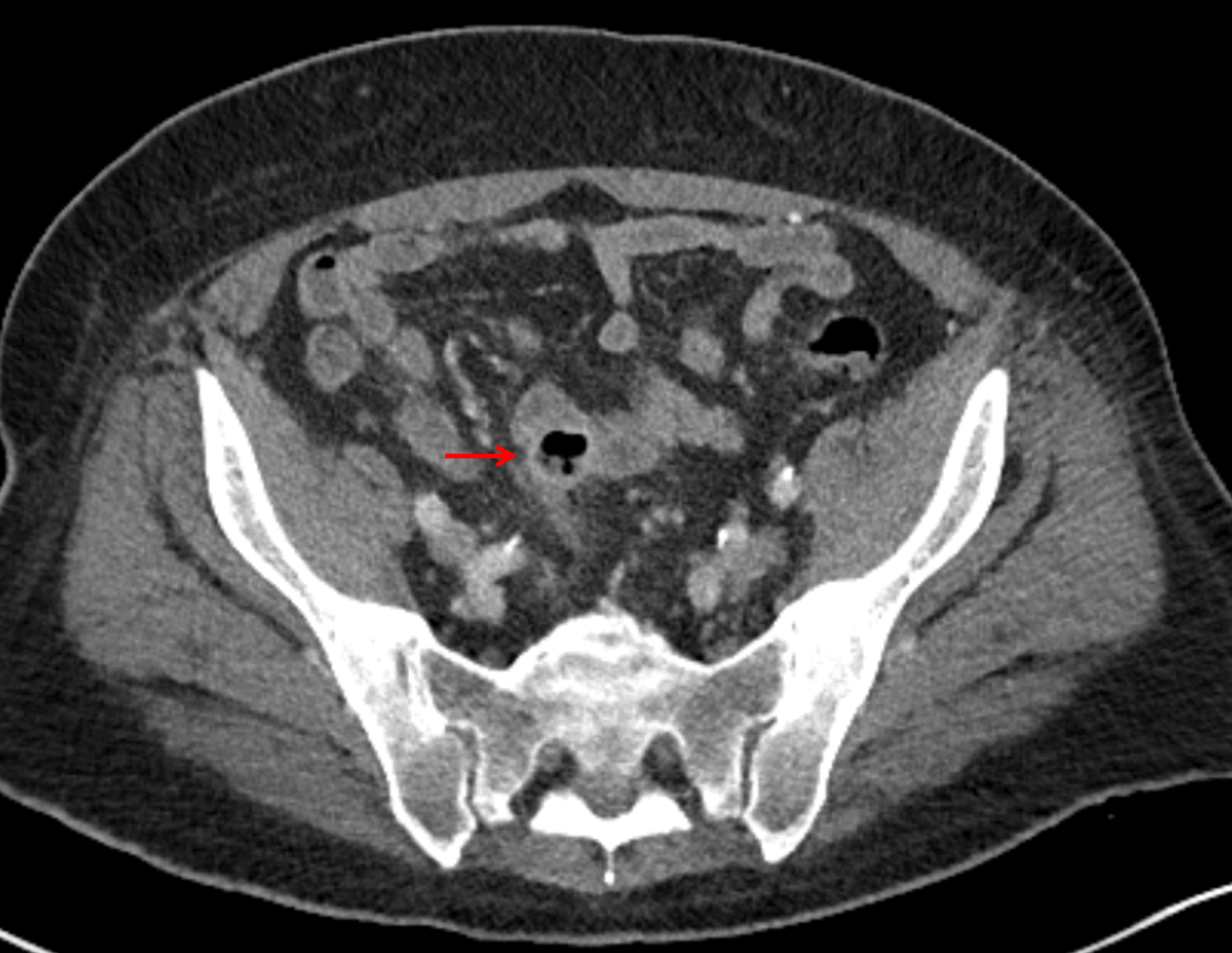
Red arrow: focal contained perforation associated with diverticulitis.