Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Findings
Chest
- Small lower anterior mediastinal hematoma without active extravasation
- Trace right pneumothorax
- Mild contusion in the anterior aspect of the left upper lobe
- Mild dependent bilateral lower lobe atelectasis
- Small hiatal hernia
Abdomen/Pelvis
- Hepatic laceration involving segments 2/3 measuring 4.4 cm in greatest span. No extension to the hilum or evidence of active hemorrhage
- Moderate volume hemoperitoneum, particularly concentrated about the liver and in the right paracolic gutter
- Stranding in the right ileocolic and left colic mesentery with areas of associated contrast density which change in size and appearance on delayed images
MSK
- Acute nondisplaced fractures of the right lateral third and fourth ribs
- Acute minimally displaced fractures through the costal cartilage of multiple right ribs
- Remote right lateral eighth and ninth rib fractures
- Acute minimally displaced fracture of the xiphoid process
- Acute minimally displaced fracture of the anterior superior corner of the L4 vertebral body
- Traumatic rupture of all fascial layers of the left lateral abdominal wall near their attachment on the left iliac crest resulting in a lumbar hernia, which only contains fat
- Intramuscular hematoma in the imaged portion of the left sternocleidomastoid muscle
- Soft tissue contusion anterior to the sternum
Diagnosis
Hepatic laceration
Mesenteric injuries with active hemorrhage
Mediastinal hematoma
Traumatic lumbar hernia
Sample Report
Traumatic hematomas in the right ileocolic and left colic mesenteries with evidence of active hemorrhage at both locations.
Grade 3 hepatic laceration in segments 2/3 with moderate volume hemoperitoneum.
Acute left lumbar hernia with herniation of abdominal fat through the defect.
Acute fractures through the right costal cartilage and xiphoid process with a small lower mediastinal hematoma. No direct evidence of acute aortic injury.
Acute nondisplaced fractures of the right lateral third and fourth ribs with a tiny right pneumothorax.
Acute minimally displaced fracture of the anterior superior corner of the L4 vertebral body.
Partially imaged intramuscular hematoma in the left sternocleidomastoid muscle.
Discussion
- Hepatic injuries can be classified using the AAST system, as shown in the table below. While including the classification of injuries is not always important, it is important to generate reports that will be meaningful to your referring surgeons.
- Any time you see a laceration or hematoma, make sure to compare closely between arterial and delayed phases for signs of arterial injury including hemorrhage (should get larger and less poorly defined on delayed phase) and pseudoaneurysm (should remain similar in appearance on delayed phase)
- When you see a laceration that extends to or near the hepatic hilum, make sure to look for biliary complications which can include:
- Hemorrhage into a bile duct causing obstruction - look for regional intrahepatic duct dilation
- Bile leak, which will initially look like nonloculated low density fluid, but will progress to a biloma over time
- This case also shows a good example of a traumatic lumbar hernia, as shown in an annotated image below. While rare, these indicate severe shearing forces and can unfortunately easily be missed by clinicians and radiologists in polytrauma cases
AAST Liver Injury Scale
Annotated Images & Illustrations
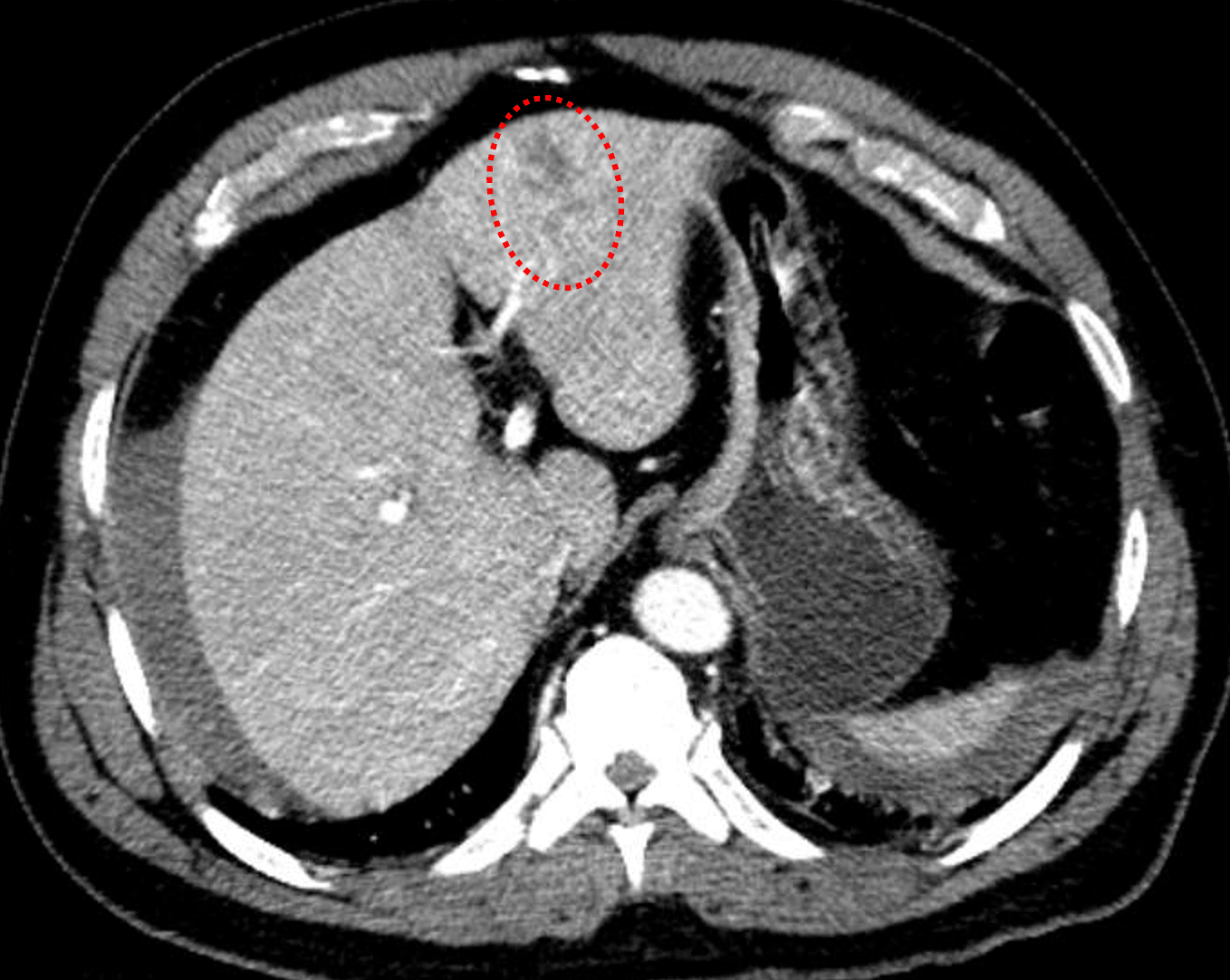
Red outline: hepatic laceration in segment 4 measuring greater than 3 cm in depth.
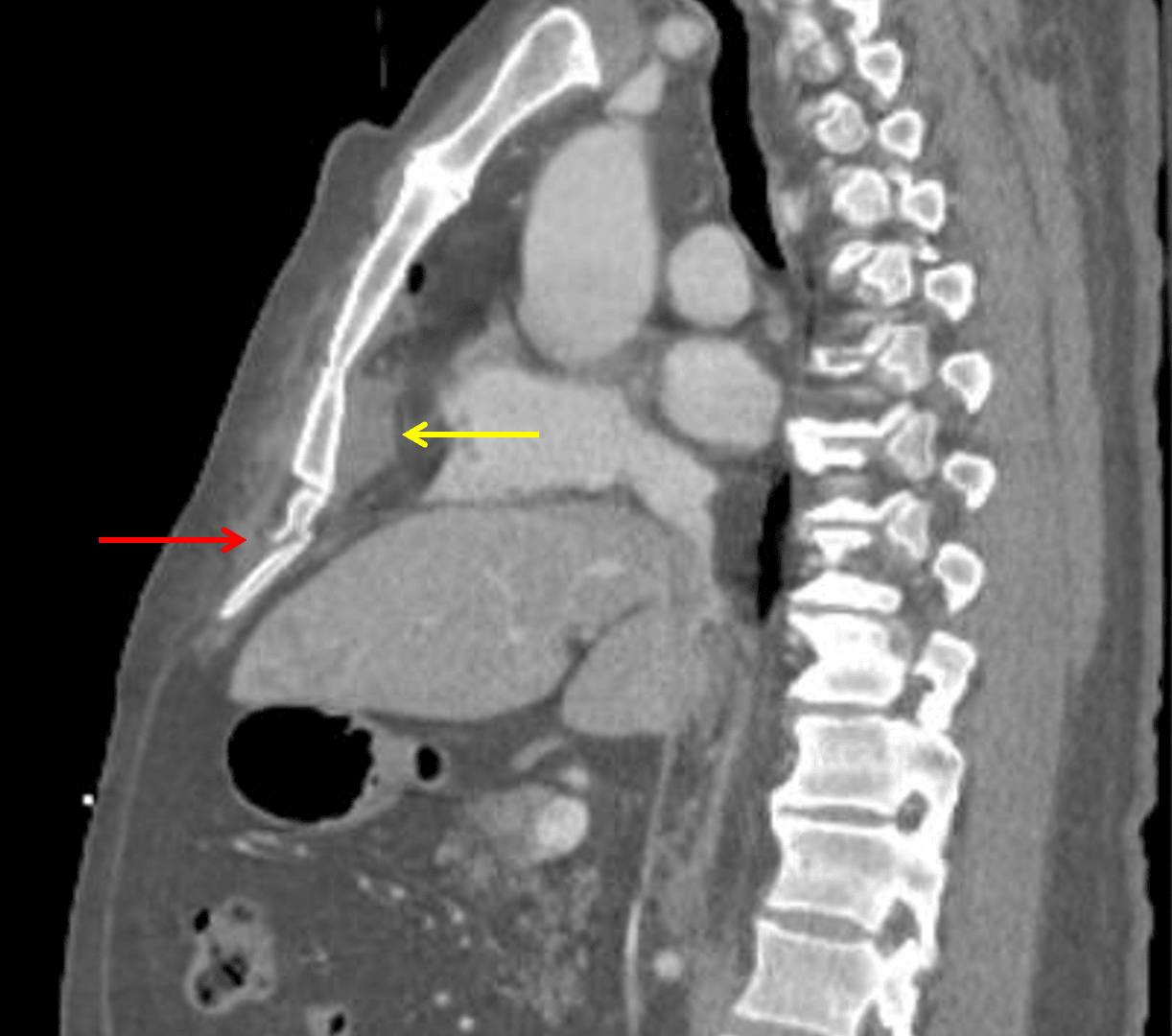
Xiphoid process fracture (red arrow) and subjacent mediastinal hematoma (yellow arrow).
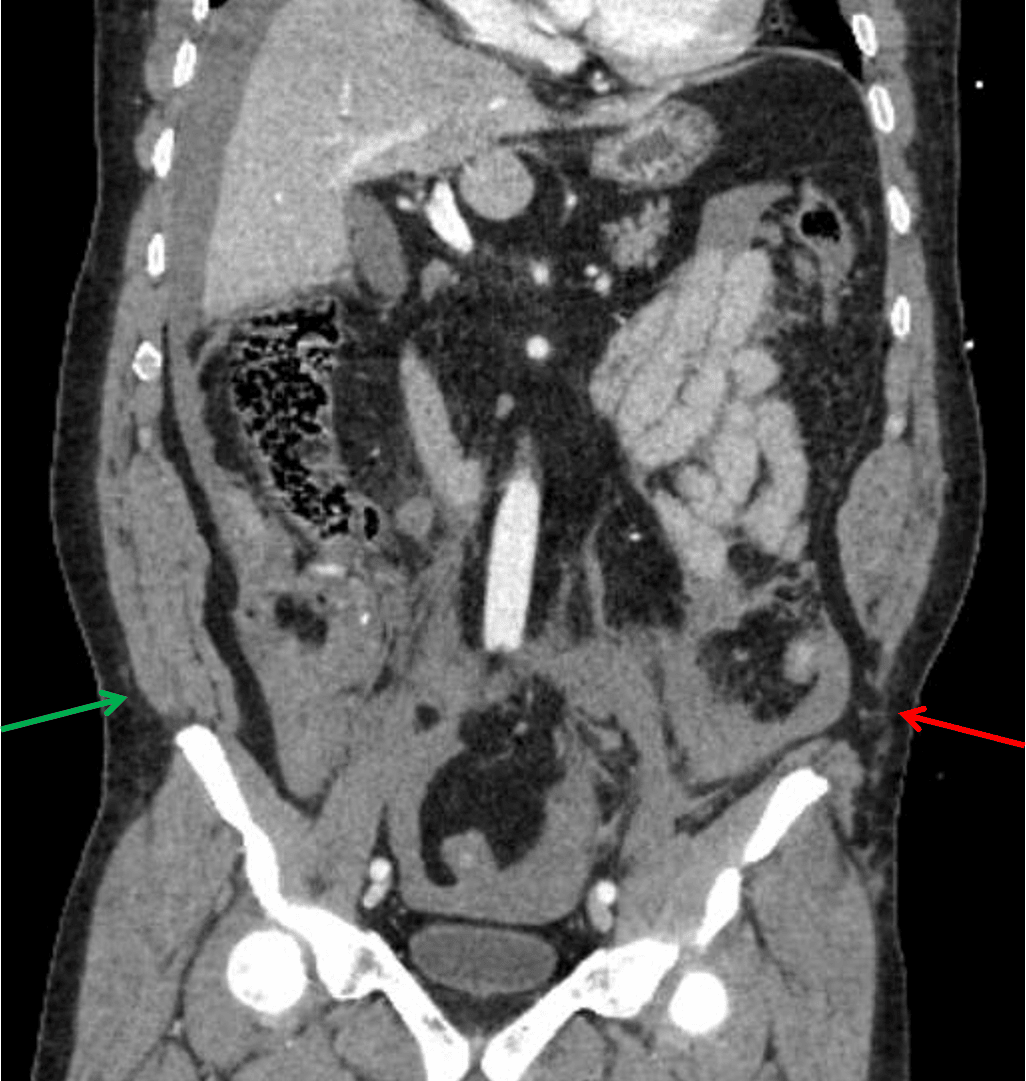
Traumatic herniation of the abdominal wall musculature from the left iliac crest (red arrow) compared to the normal appearance on the right (green arrow).