Findings
- Acute nondisplaced left parietal calvarial fracture extending into the left lambdoid suture with mild sutural diastasis
- Subjacent epidural hematoma measuring up to 2 cm in thickness
- Associated mass effect with crowding of the ambient and quadrigeminal cisterns, crowding of the fourth ventricle, and mild upward and downward bulging of the posterior fossa structures without frank herniation
- Small hemorrhagic contusion in the right anterior temporal lobe
- Left parietal scalp hematoma, a portion of which is likely subgaleal, with intermixed locules of gas
- Mucosal thickening of the paranasal sinuses with near complete opacification of the left sphenoid sinus
Diagnosis
Epidural hematoma
Sample Report
Acute nondisplaced left parietal calvarial fracture extending into the left lambdoid suture with mild sutural diastasis.
Subjacent epidural hematoma measuring up to 2 cm in thickness. Small hemorrhagic contusion in the right anterior temporal lobe compatible with contrecoup injury.
Corresponding mass effect in the posterior fossa without frank herniation or hydrocephalus at this time. However, recommend attention on short interval follow-up imaging.
Mucosal thickening of the paranasal sinuses with near complete opacification of the left sphenoid sinus, which can be seen with acute sinusitis.
Discussion
- Epidural hematomas represent bleeding between the dura and the inner table of the calvarium
- These are typically arterial, with the middle meningeal artery being the most common offender, but venous epidural hemorrhage is also possible. Here are some common locations for venous epidural hemorrhage:
- Vertex: fracture and/or sagittal suture diastasis -> superior sagittal sinus injury -> epidural hematoma crossing the suture and inferiorly displacing the sinus
- Anterior middle cranial fossa: due to hemorrhage from the sphenoparietal sinus, can be managed conservatively
- Posterior fossa adjacent to an occipital fracture: often related to sinus (especially transverse sinus) injury
- Most are associated with skull fractures
- Epidural hematomas can rapidly expand leading to herniation and death. "Swirling" low density within the hematoma (which is arguably present to some degree in this case) indicates non-clotted fresh blood mixing in with the clotted blood and is concerning for ongoing bleeding
- Epidural hematomas are less common in elderly patients due to increased adherence of the dura to the skull with age
- Epidural hematomas respect suture lines where the periosteal component of the dura extends through the skull. There is one major exception to this: if the suture is disrupted (e.g. if it is diastatic on imaging or if a fracture extends through a suture), then the hematoma can cross suture lines. Notice that the hematoma extends across the diastatic lambdoid suture in this case
- Always look for contrecoup injuries. These are most commonly seen involving the temporal poles and inferior frontal lobes
Annotated Images & Illustrations
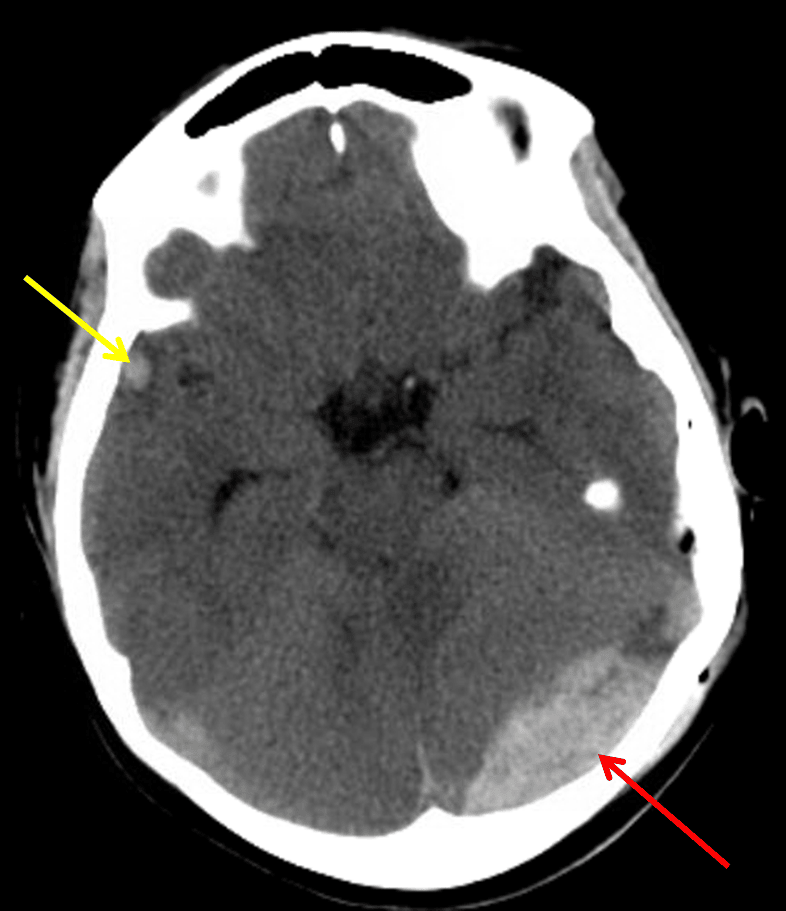
Red arrow: acute epidural hematoma. Yellow arrow: small contrecoup cerebral contusion.

Scalp hematoma with distinct deep (red arrow) and superficial (yellow arrow) components. The deep component contains layering hyperdense blood products and is likely subgaleal in location.
References