Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Findings
- Opacification and volume loss in the right upper lobe with superior displacement of the minor fissure
- Mild rightward mediastinal shift
- Mild patchy left lower lobe opacification
- Right IJ approach Port-A-Cath with tip overlying the superior cavoatrial junction
- No pleural effusion or pneumothorax
- Normal size and configuration of the cardiopericardial silhouette
Diagnosis
Right upper lobe collapse
Sample Report
Right upper lobe collapse, which raises concern for mucous plugging or a central obstructing mass. Recommend chest CT for further evaluation.
Mild patchy opacities in the left lower lobe are nonspecific and may relate to atelectasis, aspiration, or pneumonia.
Discussion
- Right upper lobe collapse is often identified on a frontal radiograph by volume loss and opacification with upward deviation of the minor fissure
- The Golden S sign results from the medial aspect of the minor fissure getting caught on a hilar mass while the mid and lateral portions elevate - so if you see this appearance, think about a central obstructing mass
Annotated Images & Illustrations
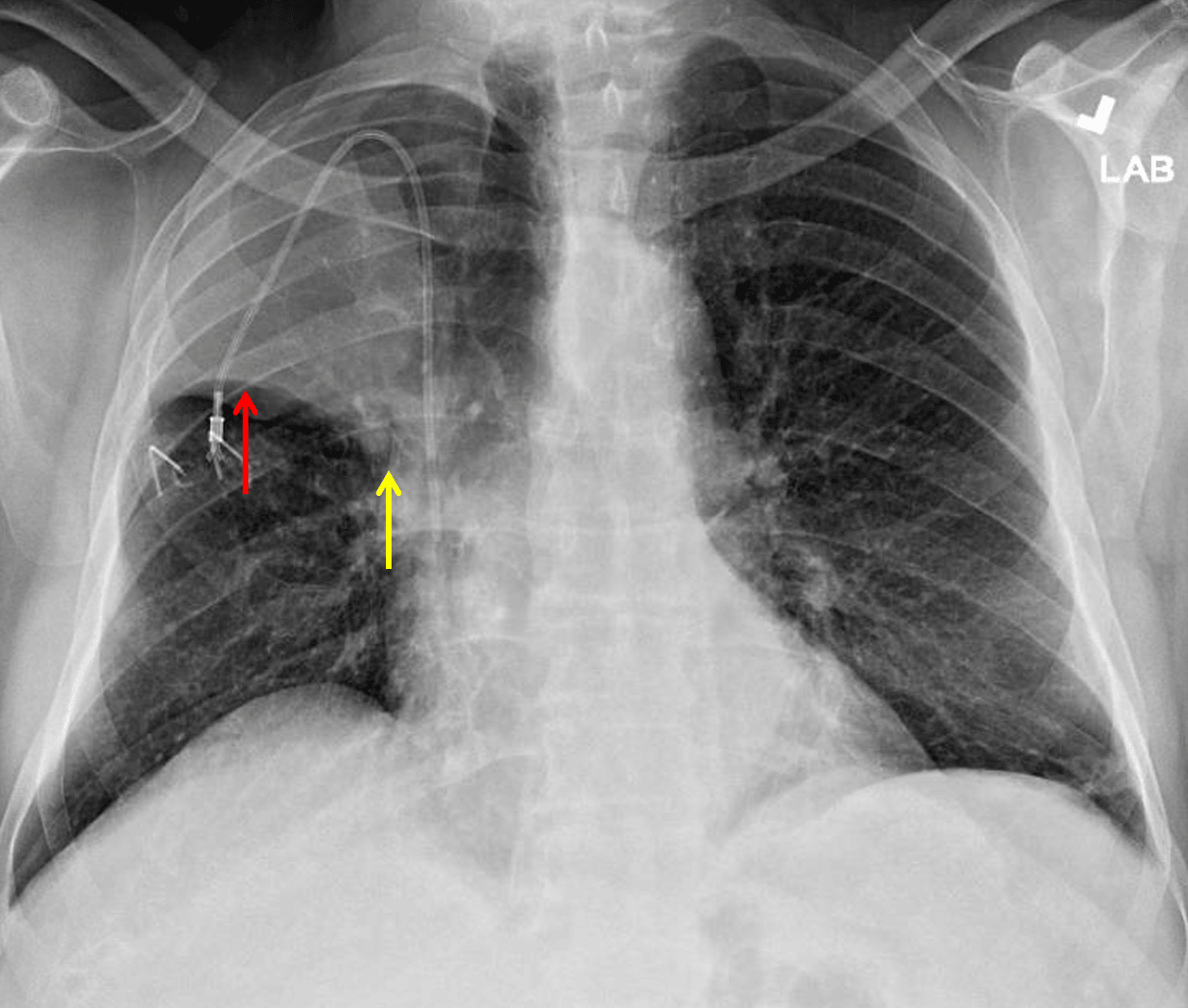
Right upper lobe collapse. The minor fissure is elevated laterally (red arrow) but not as elevated centrally (yellow arrow) raising concern for a perihilar mass.
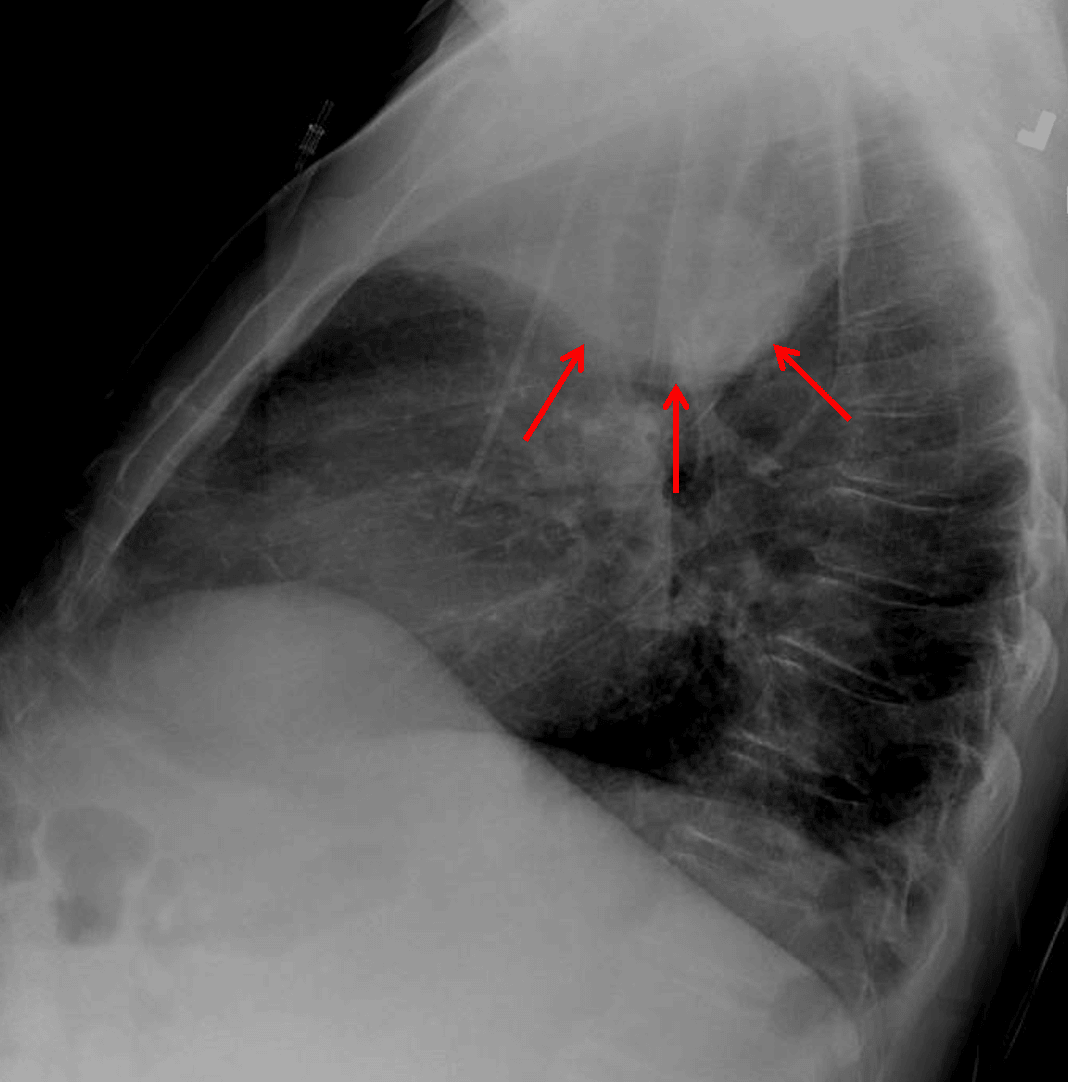
Right upper lobe collapse. Lateral view shows a paradoxical bulging appearance along the inferior margin of the collapsed lobe concerning for mass (red arrows).
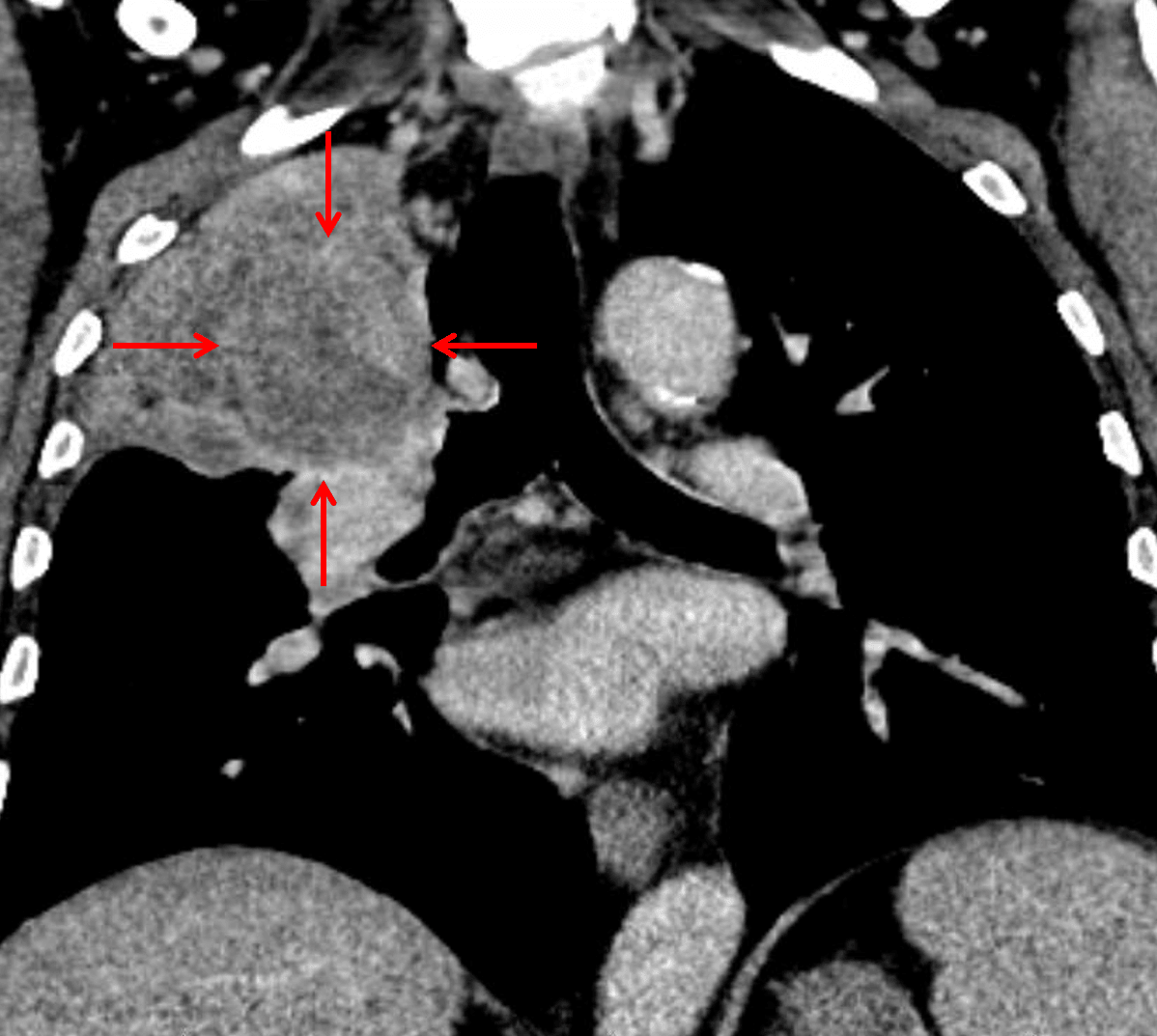
Subsequent CT confirmed the presence of a suprahilar mass with bronchial invasion (red arrows), though the mass is difficult to distinguish from the adjacent atelectatic lung.
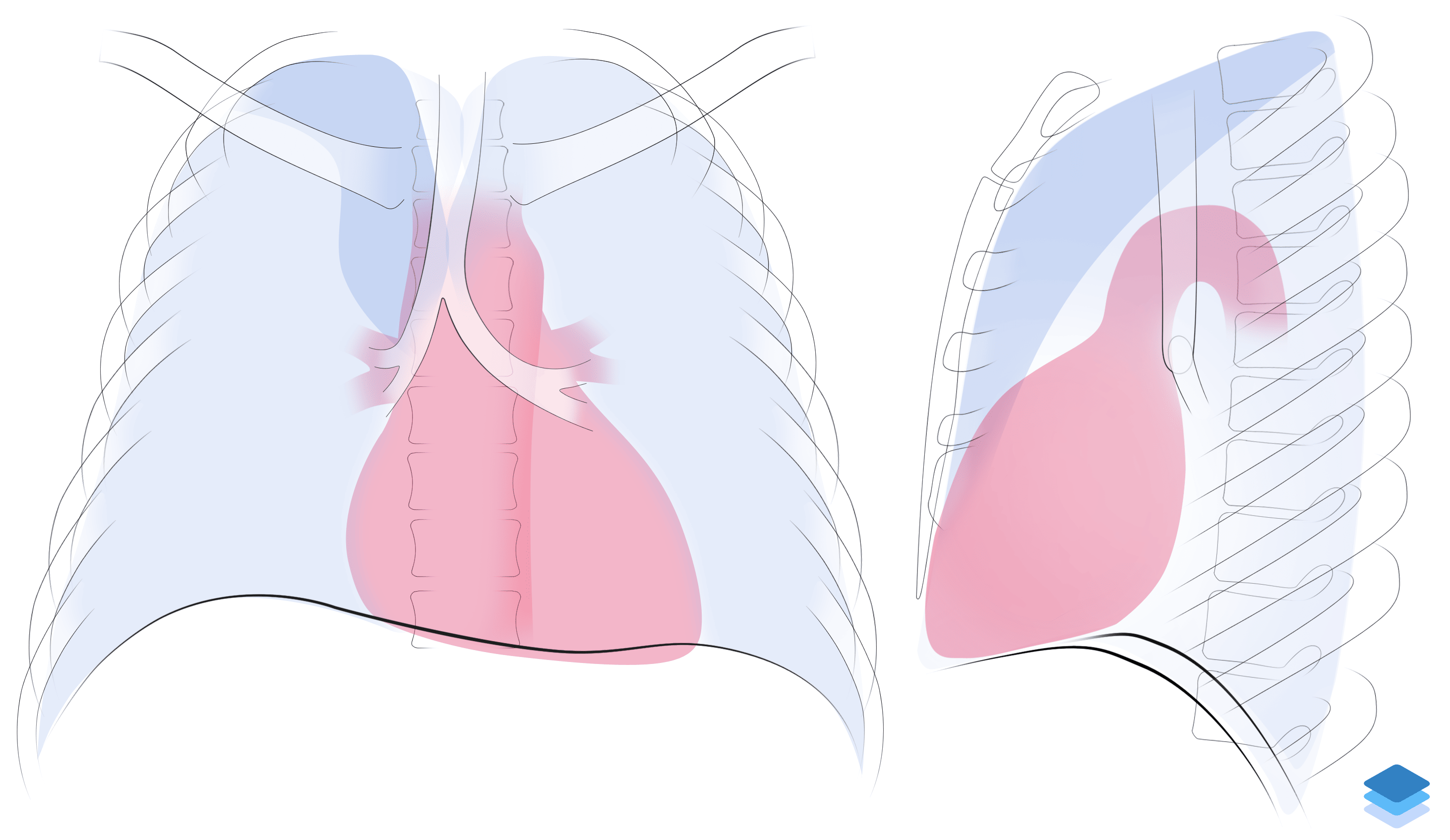
Right upper lobe collapse. Illustration by Valerie George, MD