Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Findings
Chest Radiograph
- Acute nondisplaced right first rib fracture
- No pleural effusion or pneumothorax
- Mild hazy bibasilar opacities
CT
Chest
- Mild peripheral groundglass opacities in the anterior aspects of the right upper and middle lobes and to a lesser extent in the lingula
- Trace right apical and left anterior pneumothoraces
- Trace anterior pneumomediastinum
- Residual thymus in the anterior mediastinum
Abdomen/Pelvis
- No acute findings
- Narrowing and inferior deviation at the origin of the celiac artery with poststenotic dilation
MSK
- Acute nondisplaced fractures of the right first rib and of the left fifth, sixth, seventh, and eighth ribs
- Acute L1 compression fracture with approximately 10% anterior height loss and no bony retropulsion
- Possible additional acute compression fracture of the T11 vertebral body without significant height loss or bony retropulsion
- Mild offset of the coccygeal segments
Diagnosis
Pulmonary contusion
Sample Report
Acute nondisplaced fractures of the right first and left fifth through eighth ribs.
Trace bilateral pneumothoraces.
Trace anterior pneumomediastinum without mediastinal hematoma or evidence of aortic trauma.
Pulmonary contusion in the anterior aspects of the right upper and middle lobes and to a lesser extent in the lingula.
Acute L1 and possibly T11 compression fractures with minimal height loss and no bony retropulsion.
Age-indeterminate mild offset of the coccygeal segments which may be traumatic or developmental.
No acute traumatic findings in the abdominopelvic cavity.
Narrowing at the origin of the celiac artery likely relates to median arcuate ligament compression. Though often asymptomatic, this finding can be a cause for chronic abdominal pain.
Discussion
- Pulmonary contusion is often located in a non-dependent area of the lung and correlates with the site(s) of blunt chest trauma
- Pulmonary contusion will typically resolve within a few days with supportive management, so if you see groundglass opacities persisting a week or more after trauma or appearing more than 24 hours after trauma, there is likely something else going on
- If you see bilateral dependent groundglass opacities, this is more likely to represent subsegmental atelectasis or aspiration
- Make sure to look for associated pulmonary laceration or pneumatocele
- In this case, the trace pneumomediastinum is likely a product of the Macklin effect: gas released from alveolar rupture tracks along bronchovascular bundles back to the mediastinum
- However, whenever you see pneumomediastinum, make sure to look closely for evidence of tracheobronchial or esophageal injury and look for other signs of mediastinal trauma including mediastinal hematomas and aortic injuries
Annotated Images & Illustrations
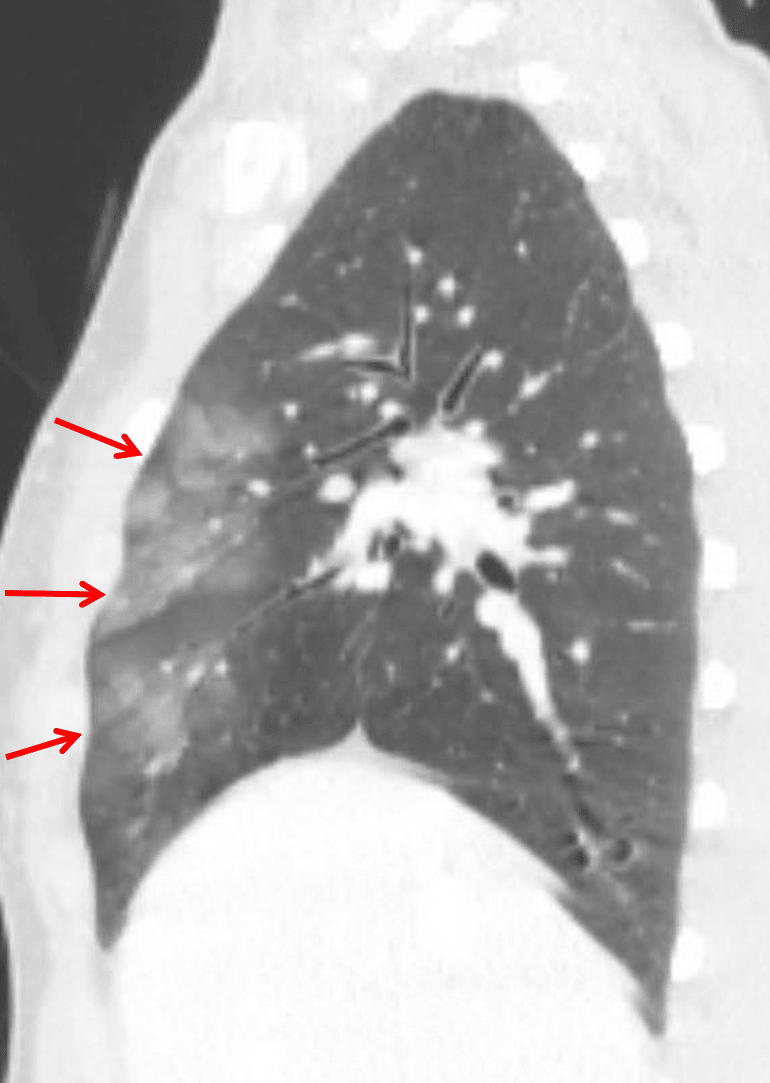
Pulmonary contusion: groundglass opacities in the anterior aspects of the right upper and middle lobes (red arrows).