Use mouse wheel, arrow keys or left click (with scroll tool selected) to scroll
ui.case.use_touch_gestures
DICOM HelpSource: Local (us-east1-c)
Findings
Lower chest
- Small right and trace left pleural effusions
- Mild dependent atelectasis
Abdomen/Pelvis
- Multifocal submucosal edema/hyperenhancement from the esophagus through the rectum with most severe involvement of the duodenum and proximal colon
- Dilated, fluid-filled lower thoracic esophagus
- Surgical changes of recent appendectomy with small volume abdominopelvic ascites, particularly in the right paracolic gutter
- Periportal edema in the liver
- Subcentimeter hepatic hypodensities, which are too small to characterize
- Mild fullness of both renal collecting systems
- Urothelial thickening and enhancement of the bilateral ureters, particularly distally
- Diffuse mesenteric edema
- Trace locules of free intraperitoneal air, including adjacent to the hepatic dome and the left portal vein
MSK
- No acute osseous findings
- Slight retrolisthesis of L5 on S1
- Body wall edema
Diagnosis
Small vessel vasculitis
Sample Report
Nonspecific multifocal submucosal edema throughout the bowel from the esophagus to the rectum with severe edema of the duodenum and proximal colon. In this patient with lupus, these findings are particularly concerning for a small vessel vasculitis. Infectious/inflammatory enteritis/colitis is also on the differential, but considered less likely given the distribution and discontinuous involvement.
Surgical changes of appendectomy without loculated intraabdominal collection. Trace intraperitoneal free air is likely postsurgical.
Distended, fluid-filled lower thoracic esophagus, which places the patient at risk for aspiration.
Findings suggestive of volume overload, including small pleural effusions, mesenteric edema, small volume abdominopelvic ascites, and body wall edema.
Mild fullness of the bilateral renal collecting systems with urothelial thickening and enhancement of both ureters. While this could be secondary to adjacent inflammation, recommend correlation with urinalysis if there is clinical concern for urinary tract infection.
Discussion
- Lupus can affect any and every organ system with pathologies resulting from immune complex deposition and vasculopathy. The reference listed below gives a good overview of the spectrum of conditions associated with lupus from a radiologist's perspective
- When the bowel is involved, it is most often the result of small vessel disease (which is not usually directly visualized on imaging) with the SMA distribution being most commonly involved
- Make sure to think about vasculitis and angioedema when you see segmental submucosal edema, particularly when the patient story is not typical for enteritis/colitis or inflammatory bowel disease
Annotated Images & Illustrations
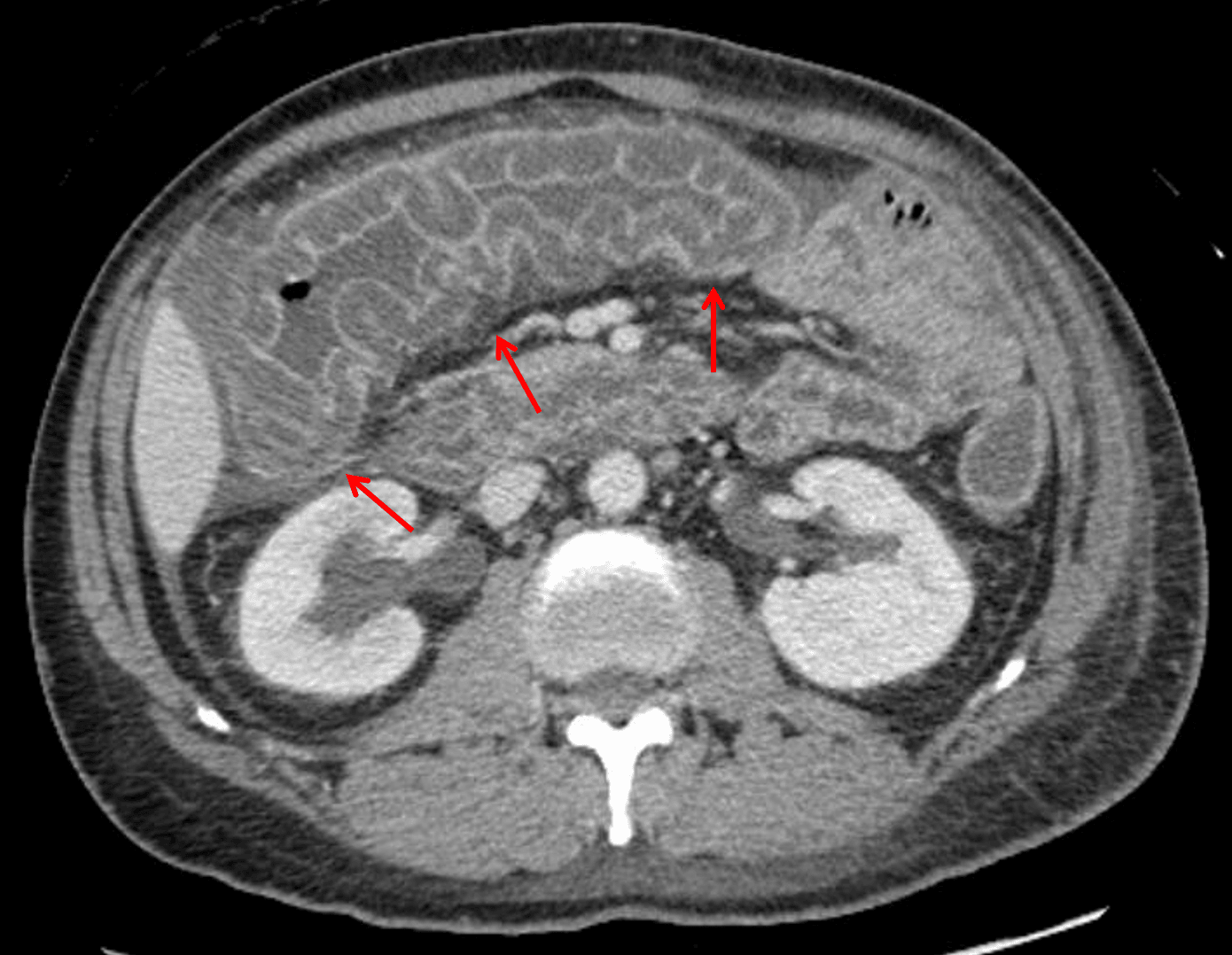
Lupus vasculitis: marked submucosal edema at the hepatic flexure and transverse colon resulting in a thumbprinting appearance of the mucosa (red arrows).